
Skincare differs by ethnicity because of measurable biological differences in melanin concentration, skin structure, and inflammatory response that directly affect how skin reacts to products, UV exposure, and treatments. These are not cosmetic distinctions. They are physiological realities backed by dermatology research, and they explain why a retinol serum that works beautifully on one person can trigger weeks of post-inflammatory hyperpigmentation on another. Understanding why skincare differs by ethnicity is the first step toward building a routine that actually works for your skin, not someone else's. Ingredients like Arbutin, Kojic Acid, and Turmeric exist precisely because melanin-rich skin has specific, evidence-based needs.
Why skincare differs by ethnicity: the biology behind it
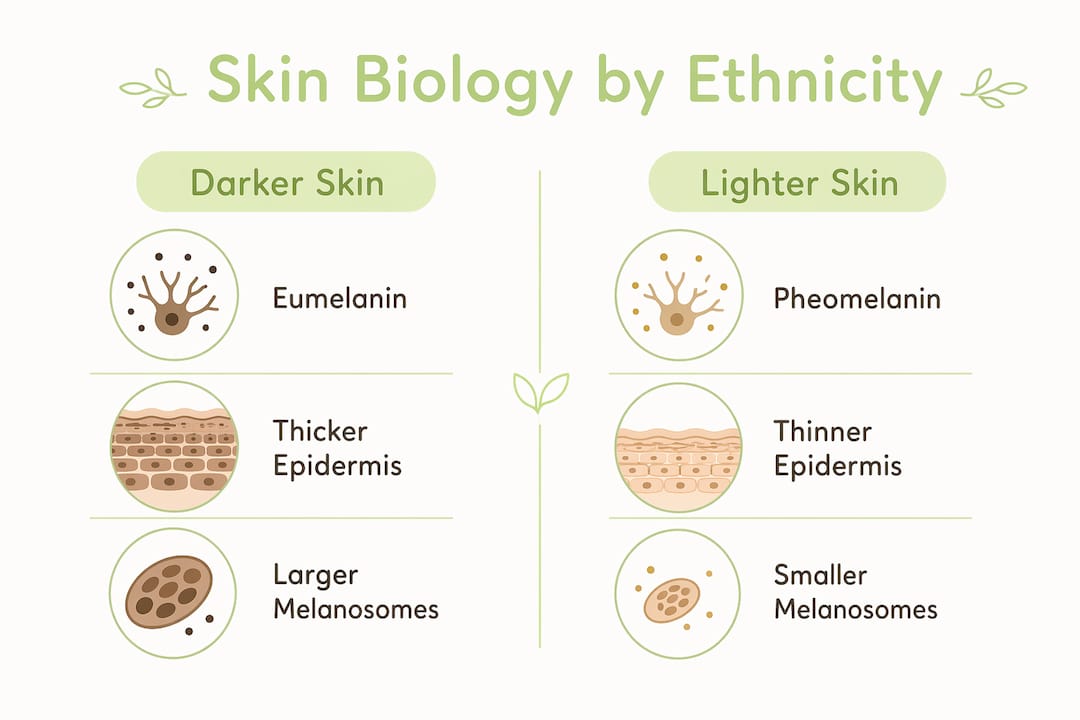
The core reason ethnic skincare routines diverge comes down to melanin. Specifically, the type, quantity, and architecture of melanin in your skin determines how your skin handles sun damage, inflammation, and pigmentation disorders. Skin contains two primary melanin types: eumelanin, which is brown to black and dominates in darker skin tones, and pheomelanin, which is yellow to red and more prevalent in lighter skin. These are not interchangeable. Eumelanin in darker skin provides stronger photoprotection and handles oxidative stress differently than pheomelanin does in lighter skin. That structural difference alone explains why two people can stand in the same sun for the same amount of time and experience completely different outcomes.
Beyond melanin type, the physical architecture matters. Darker skin contains larger, more dispersed melanosomes (the cellular packages that carry melanin), while lighter skin has smaller, clustered melanosomes. This difference in melanin distribution affects how UV radiation is absorbed and scattered at the cellular level. It also influences how the skin signals inflammation, which connects directly to the risk of post-inflammatory hyperpigmentation (PIH) after acne, injury, or aggressive treatments.

Skin structure also varies in epidermal thickness, lipid content, and transepidermal water loss rates across ethnic groups. These variations affect how well the skin barrier holds up under stress, how quickly it absorbs active ingredients, and how it responds to irritants. This is why diversity in skincare formulation is not optional. It is a clinical necessity.
What this means for photoprotection
Visible light, specifically high-energy visible light (HEVL) and UVA1, triggers melanocyte activation in ways that standard SPF ratings do not measure. Two sunscreens with identical SPF values can deliver very different pigment protection depending on whether they contain iron oxides and visible-light filters. For melanin-rich skin, this gap is clinically significant. Tinted sunscreens with iron oxides block HEVL and are now considered a standard recommendation for melasma and skin of color management, according to 2026 dermatology conference coverage. Standard untinted sunscreens, even broad-spectrum ones, leave a meaningful protection gap for darker skin tones.
Pro Tip: If you have medium to deep skin tone and are managing dark spots or melasma, switch from a clear sunscreen to a tinted formula with iron oxides. The SPF number alone does not tell you whether you are protected from the visible light that triggers pigmentation.
| Skin characteristic | Lighter phototypes | Darker phototypes |
|---|---|---|
| Primary melanin type | Pheomelanin | Eumelanin |
| Melanosome size | Small, clustered | Large, dispersed |
| UV photoprotection level | Lower | Higher |
| HEVL pigmentation risk | Moderate | High without tinted SPF |
| PIH risk after irritation | Lower | Significantly higher |
How inflammatory response varies across skin phototypes
The Fitzpatrick scale classifies skin into six phototypes based on how skin responds to UV exposure, ranging from Type I (always burns, never tans) to Type VI (never burns, deeply pigmented). What most people do not know is that Fitzpatrick phototype independently predicts short-term cutaneous reactivity after topical provocation. Lighter phototypes show higher irritant responses, while darker phototypes show minimal early reactivity to the same topical triggers. This sounds counterintuitive until you understand the downstream consequence.
Darker skin may not react visibly to an irritant right away, but when it does react, the inflammatory response is more likely to leave a lasting pigmentation mark. PIH is the skin's response to inflammation, and melanin-rich skin produces more melanin in response to injury or irritation. This means that a product causing mild redness on lighter skin can leave weeks or months of dark spots on deeper skin tones. The inflammatory threshold is different, and so is the cost of crossing it.
This has direct implications for how ethnic skincare routines should be built:
- Avoid high-concentration exfoliants (glycolic acid above 10%, strong retinoids) without a slow introduction period on deeper skin tones
- Prioritize barrier-supporting ingredients like Manuka Honey and Nano Gold that calm inflammation before it escalates
- Treat any new active ingredient as a potential PIH trigger and patch test for at least 48 hours
- Choose formulations that address inflammation and pigmentation simultaneously, since the two are biologically linked in melanin-rich skin
- Recognize that "no immediate reaction" does not mean "no reaction." Delayed responses are common in darker phototypes
Understanding this reactivity pattern is why ethnic skincare routines for deeper skin tones tend to emphasize gentler actives, consistent barrier support, and anti-inflammatory ingredients rather than aggressive exfoliation.
What pigmentary disorders look like across different ethnicities
Melasma and post-inflammatory hyperpigmentation are the two most common pigmentary concerns across all ethnicities, but they do not affect all groups equally. Melasma disproportionately affects Fitzpatrick skin types III through V and is most prevalent in reproductive-age women of Hispanic and Asian descent. Hormonal triggers, UV exposure, and genetic predisposition all contribute, but the ethnic skew is consistent across US clinical data.
Managing these conditions requires more than a single product. A 2025 global consensus developed personalized care guidelines for melanin hyperpigmentation disorders that emphasize photoprotection, topical treatments stratified by pigmentation depth, and procedural interventions calibrated to skin type. The key word is stratified. The same melasma on two different skin tones requires a different treatment algorithm.
Here is how effective pigment management is typically structured for ethnic skin:
- Assess pigmentation depth first. Superficial pigmentation responds to topical brighteners like Arbutin, Kojic Acid, and Vitamin C. Deeper dermal pigmentation requires different approaches and longer timelines.
- Lock in photoprotection before anything else. No brightening ingredient works if UV and HEVL exposure continue to stimulate melanocyte activity daily. Tinted SPF is non-negotiable.
- Introduce anti-pigmentation actives gradually. Glutathione and Kojic Acid reduce melanin synthesis at the cellular level, but aggressive use can trigger rebound pigmentation in sensitive skin.
- Control inflammation in parallel. Inflammation and photoprotection are inseparable in melasma management. Ingredients like Turmeric and Manuka Honey address the inflammatory component that drives pigment production.
- Avoid aggressive energy-based procedures without conservative protocols. Laser treatments and chemical peels carry significantly higher PIH risk in skin of color and require strict pre- and post-treatment photoprotection.
The practical takeaway: adapting skincare by ethnicity for pigment management means treating photoprotection, inflammation control, and brightening as a system, not as separate steps.
How research gaps affect skincare recommendations for diverse skin
The dermatology research base has a documented representation problem. 75% of clinical trial participants are White, which means the evidence base for treatment response, adverse effects, and product tolerance in diverse populations is structurally limited. This is not a minor data gap. It directly affects how confidently clinicians can recommend treatments for ethnic skin and how accurately adverse events are recognized and managed.
The downstream effect reaches consumers. When a product is tested primarily on lighter skin, its safety and efficacy data may not translate to melanin-rich skin. Side effects that appear minor in lighter phototypes (mild redness, slight peeling) can manifest as significant PIH in darker skin. Clinicians trained on homogeneous data sets may also underdiagnose or misread pigmentation changes in skin of color.
| Research factor | Current state | Impact on ethnic skincare |
|---|---|---|
| Trial participant diversity | 75% White participants | Limited efficacy data for skin of color |
| Adverse event recognition | Calibrated to lighter skin | PIH and reactions may be missed in darker tones |
| Pigmentation classification | Often race-based (subjective) | Inaccurate; objective ITA measurement is more reliable |
| Clinician training | Underrepresents skin of color | Lower diagnosis confidence for ethnic skin conditions |
One critical distinction that better-trained clinicians make is between constitutive pigmentation (your baseline genetic skin color) and facultative pigmentation (changes caused by sun, hormones, or inflammation). The same visible dark spot can have entirely different underlying causes, and treating them identically produces inconsistent results. Objective measurement tools like the Individual Typology Angle (ITA) give a more accurate read of actual pigmentation than racial self-identification alone.
Pro Tip: When evaluating a skincare product's clinical claims, check whether the study included participants with Fitzpatrick types IV through VI. If the trial was conducted exclusively on lighter skin, the results may not apply to you.
Key takeaways
Effective skincare for diverse ethnicities requires tailored photoprotection, inflammation management, and pigment-specific actives working together as a system, not as isolated steps.
| Point | Details |
|---|---|
| Melanin type drives skin behavior | Eumelanin in darker skin offers stronger UV protection but increases PIH risk when inflamed. |
| Tinted SPF is non-negotiable | Iron oxide sunscreens block HEVL that standard SPF formulas miss, critical for melanin-rich skin. |
| Fitzpatrick phototype predicts reactivity | Lighter skin reacts faster to irritants; darker skin reacts later but with higher pigmentation consequences. |
| Research gaps affect product safety | With 75% White trial participants, efficacy and adverse event data for ethnic skin remains limited. |
| Pigment management requires a system | Photoprotection, inflammation control, and brightening actives must work together for lasting results. |
What I've learned about building skincare that actually works for melanin-rich skin
Most skincare advice treats ethnicity as a marketing category rather than a biological reality. That frustrates me, because the science is clear and the stakes are real. When someone with deep skin tone uses an aggressive exfoliant without barrier support and ends up with PIH that takes six months to fade, that is not a product failure. It is a formulation and education failure.
The distinction between constitutive and facultative pigmentation is one of the most underused tools in consumer skincare. Your baseline skin color is genetic and fixed. The dark spots from last year's breakout are facultative, driven by inflammation, and they respond to targeted ingredients. Treating both the same way wastes time and money. Knowing which type of pigmentation you are dealing with changes everything about which actives to reach for and in what order.
I also think the photoprotection conversation in the US is years behind where it needs to be. The SPF number on a bottle tells you almost nothing about visible light protection. For anyone managing melasma or PIH, that gap in protection is the reason progress stalls despite consistent product use. Tinted formulas with iron oxides are not a trend. They are a clinical requirement for melanin-rich skin.
The brands and formulations that get this right are the ones that start with biology, not aesthetics. That means choosing ingredients with documented mechanisms, not just good marketing. Arbutin inhibits tyrosinase. Glutathione shifts melanin synthesis toward lighter pheomelanin. Kojic Acid chelates copper ions that activate melanin production. These are not buzzwords. They are mechanisms, and they matter.
— Variety
Skincare built for your skin, not the average
If you have been piecing together a routine from products that were not designed with your skin in mind, Variety-express was built to close that gap. Every formula in the Variety-express line targets the specific concerns that matter most to melanin-rich skin: hyperpigmentation, dark spots, uneven tone, and acne scars. Active ingredients like Arbutin, Glutathione, Kojic Acid, Vitamin C, Nano Gold, Manuka Honey, and Turmeric are not decorative additions. They are the reason the formulas work.
The full range sits between $10 and $30, making consistent, evidence-based skincare accessible without compromise. Whether you are starting with a brightening soap or building a complete routine, explore the full collection at Variety-express and find what your skin has been asking for. Express Yourself.
FAQ
Why does melanin type affect skincare product choice?
Eumelanin, dominant in darker skin, handles UV stress differently than pheomelanin and produces more pigment in response to inflammation. This means darker skin tones need anti-inflammatory and brightening actives that address PIH risk, not just UV protection.
What is post-inflammatory hyperpigmentation and who is most at risk?
Post-inflammatory hyperpigmentation is dark discoloration left after skin inflammation or injury, caused by excess melanin production. People with Fitzpatrick skin types III through VI are at significantly higher risk because their skin produces more melanin in response to irritation.
Do all sunscreens protect ethnic skin equally?
No. Two sunscreens with the same SPF can deliver different pigment protection based on whether they contain iron oxides that block visible light. Tinted sunscreens are clinically recommended for melanin-rich skin managing melasma or hyperpigmentation.
Why is melasma more common in certain ethnic groups?
Melasma disproportionately affects women of Hispanic and Asian descent with Fitzpatrick types III through V due to a combination of genetic predisposition, hormonal factors, and higher melanocyte reactivity to UV and visible light exposure.
How do research gaps affect skincare safety for diverse skin tones?
With 75% of dermatology trial participants being White, adverse event data and efficacy results for darker skin tones are limited. This means some products marketed as safe may carry unrecognized risks for melanin-rich skin.